
PAM50 Intrinsic Subtype Profiles in Primary and Metastatic Breast Cancer Show a Significant Shift toward More Aggressive Subtypes with Prognostic Implications

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
2.2. Macrodissection of Tumor Tissue and RNA Isolation
2.3. Gene Expression Assay
2.4. Molecular Subtype Classification
2.5. Statistical Analysis
3. Results
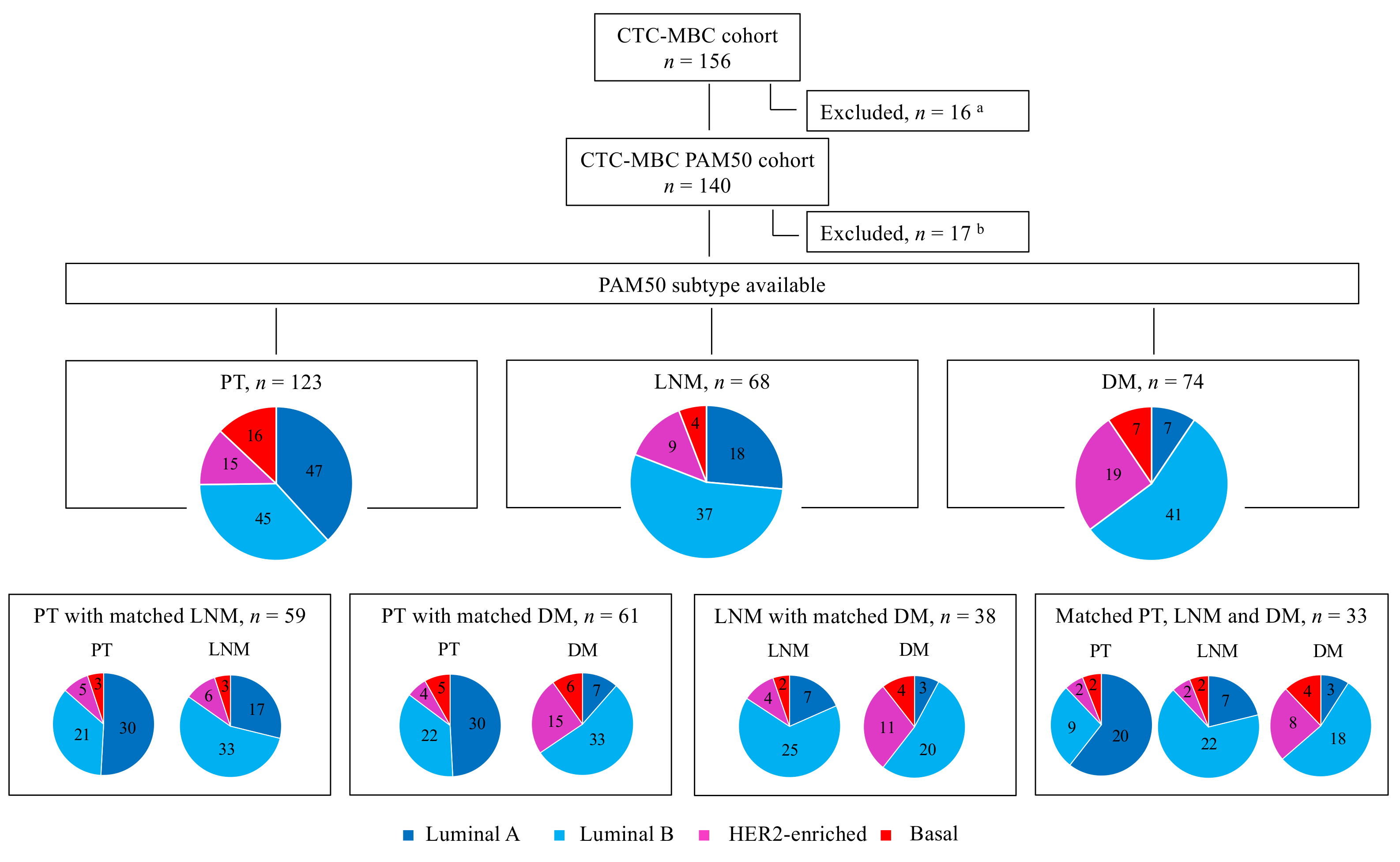
3.1. Patients and Tumor Characteristics
3.2. PAM50 Breast Cancer Intrinsic Subtype Distribution and Association with Clinicopathologic Characteristics
3.3. Concordance between PAM50 Breast Cancer Intrinsic Subtypes and Clinically Defined ER and HER2 Expression Status
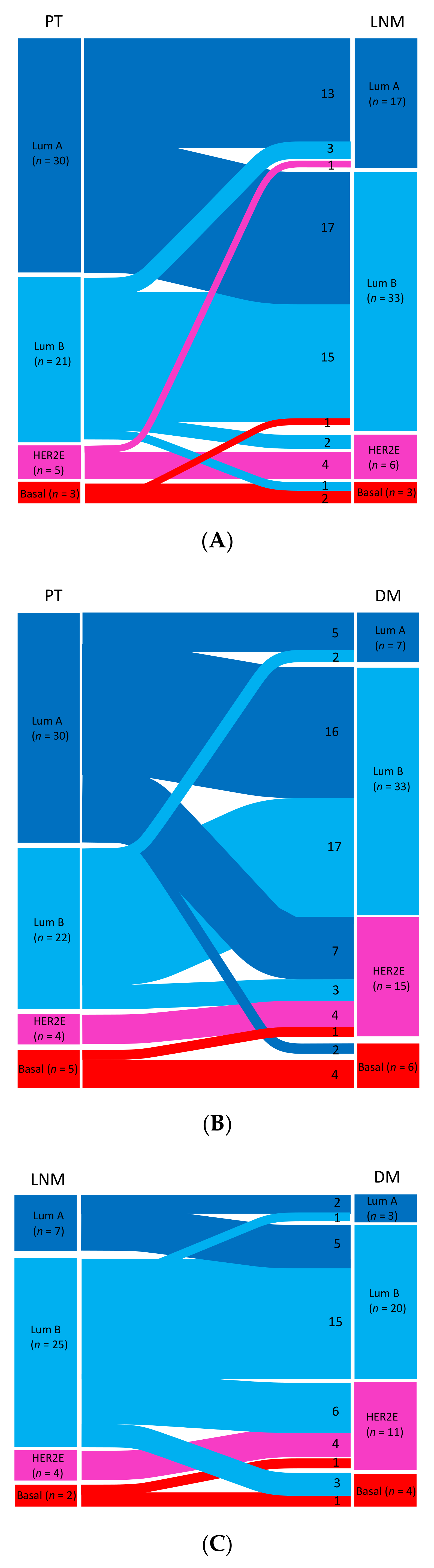
3.4. PAM50 Breast Cancer Intrinsic Subtype Status across Tumor Progression Stages in Matched Samples
3.4.1. Primary Tumors versus Matched Samples of Lymph Node Metastases
3.4.2. Primary Tumors versus Matched Samples of Distant Metastases
3.4.3. Lymph Node Metastases versus Matched Samples of Distant Metastases
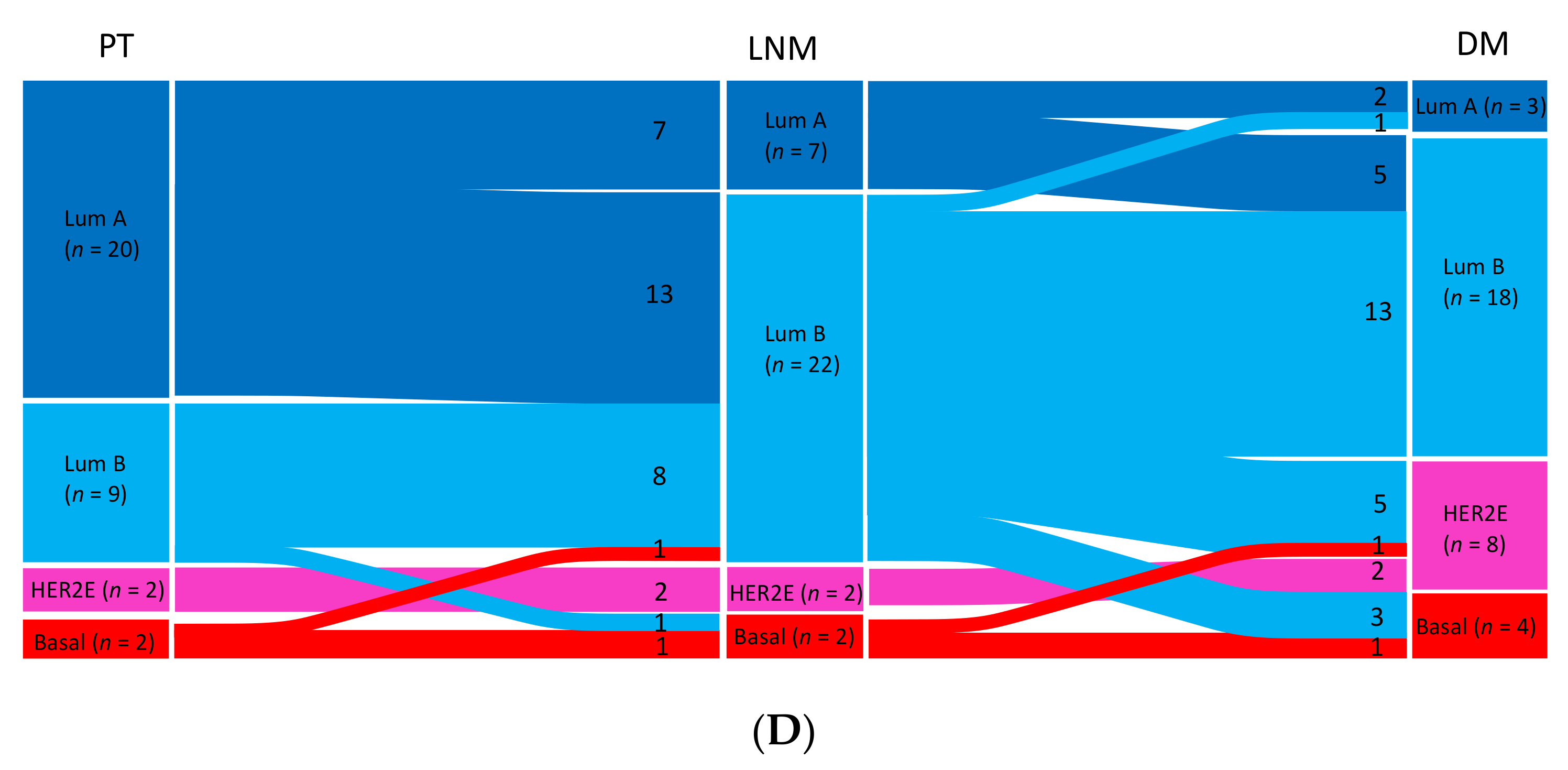
3.4.4. Primary Tumors versus Matched Samples of Lymph Node Metastases and Distant Metastases
3.5. Comparing PAM50 Breast Cancer Intrinsic Subtype Shifts from Luminal to Non-Luminal Subtypes between Tumor Sites
3.6. Associations between PAM50 Breast Cancer Intrinsic Subtype Shifts and Adjuvant Therapy
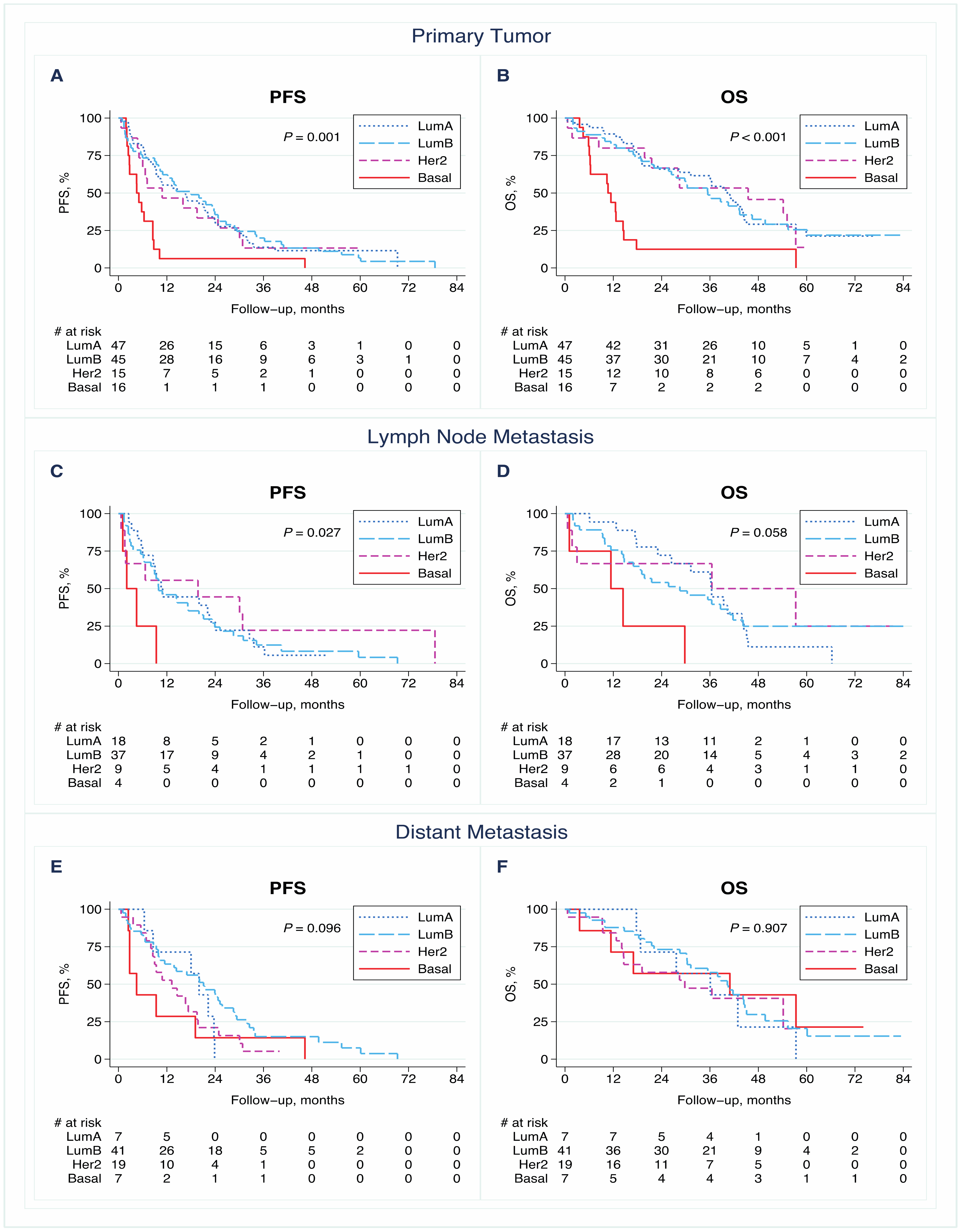
3.7. PAM50 Breast Cancer Intrinsic Subtype Status and Outcome in Patients with Available Subtype Assignment in PT, LNM, and DM
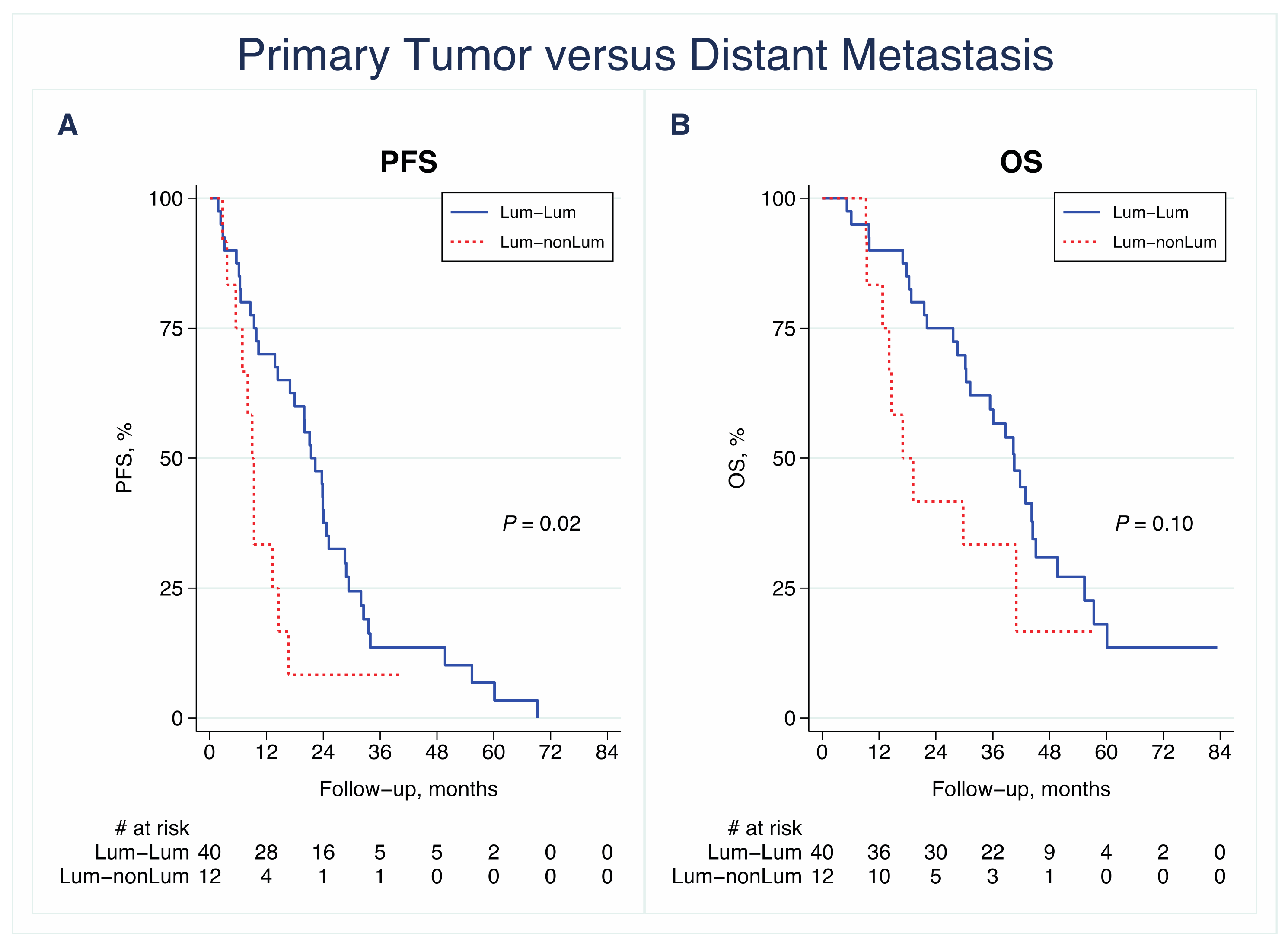
3.8. PAM50 Breast Cancer Intrinsic Subtype Shifts and Outcome in Patients with Paired Samples
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dillekås, H.; Rogers, M.S.; Straume, O. Are 90% of deaths from cancer caused by metastases? Cancer Med. 2019, 8, 5574–5576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, A.; Gao, R.; Navin, N. Tumor evolution: Linear, branching, neutral or punctuated? Biochim. Biophys. Acta Bioenerg. 2017, 1867, 151–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, C.; Papadaki, A.; Althobiti, M.; Alsaleem, M.; Aleskandarany, M.A.; Rakha, E.A. Breast cancer intratumour heterogeneity: Current status and clinical implications. Histopathology 2018, 73, 717–731. [Google Scholar] [CrossRef]
- Kimbung, S.; Loman, N.; Hedenfalk, I. Clinical and molecular complexity of breast cancer metastases. Semin. Cancer Biol. 2015, 35, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Aurilio, G.; Disalvatore, D.; Pruneri, G.; Bagnardi, V.; Viale, G.; Curigliano, G.; Adamoli, L.; Munzone, E.; Sciandivasci, A.; De Vita, F.; et al. A meta-analysis of oestrogen receptor, progesterone receptor and human epidermal growth factor receptor 2 discordance between primary breast cancer and metastases. Eur. J. Cancer 2014, 50, 277–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, M.C.; Simpson, P.T.; Reid, L.E.; Jayanthan, J.; Skerman, J.; Song, S.; Reed, A.E.M.; Kutasovic, J.R.; Morey, A.L.; Marquart, L.; et al. Metastatic progression of breast cancer: Insights from 50 years of autopsies. J. Pathol. 2014, 232, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Schrijver, W.; Suijkerbuijk, K.P.M.; van Gils, C.H.; van der Wall, E.; Moelans, C.B.; van Diest, P.J. Receptor Conversion in Distant Breast Cancer Metastases: A Systematic Review and Meta-analysis. J. Natl. Cancer Inst. 2018, 110, 568–580. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Senkus, E.; Costa, A.; Papadopoulos, E.; Aapro, M.; Andre, F.; Harbeck, N.; Lopez, B.A.; Barrios, C.H.; Bergh, J.; et al. 4th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4) dagger. Ann. Oncol. 2018, 29, 1634–1657. [Google Scholar] [CrossRef] [PubMed]
- Kimbung, S.; Kovács, A.; Danielsson, A.; Bendahl, P.-O.; Lövgren, K.; Stolt, M.F.; Tobin, N.P.; Lindström, L.; Bergh, J.; Einbeigi, Z.; et al. Contrasting breast cancer molecular subtypes across serial tumor progression stages: Biological and prognostic implications. Oncotarget 2015, 6, 33306–33318. [Google Scholar] [CrossRef] [PubMed]
- Falck, A.K.; Bendahl, P.O.; Chebil, G.; Olsson, H.; Ferno, M.; Ryden, L. Biomarker expression and St Gallen molecular subtype classification in primary tumours, synchronous lymph node metastases and asynchronous relapses in primary breast cancer patients with 10 years’ follow-up. Breast Cancer Res. Treat. 2013, 140, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Falck, A.K.; Ferno, M.; Bendahl, P.O.; Ryden, L. St Gallen molecular subtypes in primary breast cancer and matched lymph node metastases—Aspects on distribution and prognosis for patients with luminal A tumours: Results from a prospective randomised trial. BMC Cancer 2013, 13, 558. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Park, K.; Lee, E.; Ahn, T.; Jung, H.H.; Lim, S.H.; Hong, M.; Do, I.-G.; Cho, E.Y.; Kim, D.-H.; et al. Gene Expression Profiling of Breast Cancer Brain Metastasis. Sci. Rep. 2016, 6, 28623. [Google Scholar] [CrossRef] [Green Version]
- Cejalvo, J.M.; De Dueñas, E.M.; Galván, P.; García-Recio, S.; Gasión, O.B.; Paré, L.; Antolín, S.; Martinello, R.; Blancas, I.; Adamo, B.; et al. Intrinsic Subtypes and Gene Expression Profiles in Primary and Metastatic Breast Cancer. Cancer Res. 2017, 77, 2213–2221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Priedigkeit, N.; Hartmaier, R.J.; Chen, Y.; Vareslija, D.; Basudan, A.; Watters, R.J.; Thomas, R.; Leone, J.P.; Lucas, P.C.; Bhargava, R.; et al. Intrinsic Subtype Switching and Acquired ERBB2/HER2 Amplifications and Mutations in Breast Cancer Brain Metastases. JAMA Oncol. 2017, 3, 666–671. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Goodison, S.; Sun, Y. Molecular profiles of matched primary and metastatic tumor samples support a linear evolutionary model of breast cancer. Cancer Res. 2020, 80. [Google Scholar] [CrossRef]
- Lluch, A.; Gonzalez-Angulo, A.M.; Casadevall, D.; Eterovic, A.K.; de Duenas, E.M.; Zheng, X.; Guerrero-Zotano, Á.; Liu, S.; Pérez, R.; Chen, K.; et al. Dynamic clonal remodelling in breast cancer metastases is associated with subtype conversion. Eur. J. Cancer 2019, 120, 54–64. [Google Scholar] [CrossRef]
- Woo, J.W.; Chung, Y.R.; Ahn, S.; Kang, E.; Kim, E.-K.; Kim, S.H.; Kim, J.H.; Kim, I.A.; Park, S.Y. Changes in Biomarker Status in Metastatic Breast Cancer and Their Prognostic Value. J. Breast Cancer 2019, 22, 439–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, R.M.; Paik, S.; Hayes, D.F. Use of Archived Specimens in Evaluation of Prognostic and Predictive Biomarkers. J. Natl. Cancer Inst. 2009, 101, 1446–1452. [Google Scholar] [CrossRef] [Green Version]
- Larsson, A.-M.; Jansson, S.; Bendahl, P.-O.; Jörgensen, C.L.T.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.; Rydén, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res. 2018, 20, 48. [Google Scholar] [CrossRef] [PubMed]
- Geiss, G.K.; Bumgarner, R.E.; Birditt, B.; Dahl, T.; Dowidar, N.; Dunaway, D.L.; Fell, H.P.; Ferree, S.; George, R.D.; Grogan, T.; et al. Direct multiplexed measurement of gene ex-pression with color-coded probe pairs. Nat. Biotechnol. 2008, 26, 317–325. [Google Scholar] [CrossRef]
- Parker, J.S.; Mullins, M.; Cheang, M.C.; Leung, S.; Voduc, D.; Vickery, T.; Davies, S.; Fauron, C.; He, X.; Hu, Z.; et al. Supervised Risk Predictor of Breast Cancer Based on Intrinsic Subtypes. J. Clin. Oncol. 2009, 27, 1160–1167. [Google Scholar] [CrossRef]
- Bidard, F.-C.; Peeters, D.J.; Fehm, T.; Nolé, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Benjamin, D.J.; Berger, J.O.; Johannesson, M.; Nosek, B.A.; Wagenmakers, E.-J.; Berk, R.; Bollen, K.A.; Brembs, B.; Brown, L.; Camerer, C.; et al. Redefine statistical significance. Nat. Hum. Behav. 2018, 2, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and Elaboration. PLoS Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [Green Version]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting recommendations for tumor MARK-er prognostic studies (REMARK). Breast Cancer Res. Treat. 2006, 100, 229–235. [Google Scholar] [CrossRef]
- Kumar, N.; Zhao, D.; Bhaumik, D.; Sethi, A.; Gann, P.H. Quantification of intrinsic subtype ambiguity in Luminal A breast cancer and its relationship to clinical outcomes. BMC Cancer 2019, 19, 215. [Google Scholar] [CrossRef]
- Yeo, S.K.; Guan, J.-L. Breast Cancer: Multiple Subtypes within a Tumor? Trends Cancer 2017, 3, 753–760. [Google Scholar] [CrossRef]
- Turner, N.C.; Reis-Filho, J.S. Genetic heterogeneity and cancer drug resistance. Lancet Oncol. 2012, 13, e178–e185. [Google Scholar] [CrossRef]
- Sorlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Sorlie, T.; Tibshirani, R.; Parker, J.; Hastie, T.; Marron, J.S.; Nobel, A.; Deng, S.; Johnsen, H.; Pesich, R.; Geisler, S.; et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc. Natl. Acad. Sci. USA 2003, 100, 8418–8423. [Google Scholar] [CrossRef] [Green Version]
- Jiang, T.; Shi, W.; Natowicz, R.; Ononye, S.N.; Wali, V.B.; Kluger, Y.; Pusztai, L.; Hatzis, C. Statistical measures of transcriptional diversity capture genomic heterogeneity of cancer. BMC Genom. 2014, 15, 876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciriello, G.; Sinha, R.; Hoadley, K.A.; Jacobsen, A.S.; Reva, B.; Perou, C.M.; Sander, C.; Schultz, N. The molecular diversity of Luminal A breast tumors. Breast Cancer Res. Treat. 2013, 141, 409–420. [Google Scholar] [CrossRef] [Green Version]
- Prat, A.; Cheang, M.C.; Galvan, P.; Nuciforo, P.; Pare, L.; Adamo, B.; Muñoz, M.; Viladot, M.; Press, M.F.; Gagnon, R.; et al. Prognostic Value of Intrinsic Subtypes in Hormone Receptor-Positive Metastatic Breast Cancer Treated with Letrozole with or without Lapatinib. JAMA Oncol. 2016, 2, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, C.; Nielsen, T.; Bjerre, K.; Liu, S.; Wallden, B.; Balslev, E.; Nielsen, D.; Ejlertsen, B. Abstract P3-06-03: Association between PAM50 breast cancer intrinsic subtypes and effect of gemcitabine in advanced breast cancer patients. Poster Sess. Abstr. 2012, 53, 776–787. [Google Scholar] [CrossRef]
- Falato, C.; Tobin, N.P.; Lorent, J.; Lindström, L.S.; Bergh, J.; Foukakis, T. Intrinsic subtypes and genomic signatures of primary breast cancer and prognosis after systemic relapse. Mol. Oncol. 2015, 10, 517–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prat, A.; Tsai, Y.-H.; Pascual, T.; Paré, L.; Adamo, B.; Vidal, M.; Brasó-Maristany, F.; Galván, P.; Brase, J.C.; Rodrik-Outmezguine, V.; et al. A Prognostic Model Based on PAM50 and Clinical Variables (PAM50MET) for Metastatic Hormone Receptor–positive HER2-negative Breast Cancer. Clin. Cancer Res. 2020, 26, 6141–6148. [Google Scholar] [CrossRef]
- Tobin, N.P.; Harrell, J.C.; Lovrot, J.; Brage, S.E.; Stolt, M.F.; Carlsson, L.; Einbeigi, Z.; Linderholm, B.; Loman, N.; Malmberg, M.; et al. Molecular subtype and tumor characteristics of breast cancer metastases as assessed by gene expression significantly influence patient post-relapse survival. Ann. Oncol. 2015, 26, 81–88. [Google Scholar] [CrossRef]
- Tobin, N.P.; Lundberg, A.; Lindström, L.S.; Harrell, J.C.; Foukakis, T.; Carlsson, L.; Einbeigi, Z.; Linderholm, B.K.; Loman, N.; Malmberg, M.; et al. PAM50 Provides Prognostic Information When Applied to the Lymph Node Metastases of Advanced Breast Cancer Patients. Clin. Cancer Res. 2017, 23, 7225–7231. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PAM50 Subtype Available n (%) | Lum A n (%) | Lum B n (%) | HER2-E n (%) | Basal-Like n (%) | pa |
|---|---|---|---|---|---|---|
| All | 123 | 47 | 45 | 15 | 16 | |
| Age at MBC diagnosis (years) | 0.20 d | |||||
| <65 | 63 (51) | 22 (47) | 20 (44) | 10 (67) | 11 (69) | |
| ≥65 | 60 (49) | 25 (53) | 25 (56) | 5 (33) | 5 (31) | |
| ECOG (BL) | 0.10 e | |||||
| 0 | 70 (58) | 34 (75) | 21 (48) | 7 (47) | 8 (50) | |
| 1 | 31 (26) | 8 (18) | 14 (32) | 5 (33) | 4 (25) | |
| 2 | 19 (16) | 3 (7) | 9 (20) | 3 (20) | 4 (25) | |
| Missing | 3 | 2 | 1 | 0 | 0 | |
| Size (PT) | 0.77 e | |||||
| T1 | 38 (33) | 15 (33) | 13 (29) | 3 (27) | 7 (43) | |
| T2 | 43 (37) | 17 (38) | 18 (40) | 5 (46) | 3 (19) | |
| T3 | 19 (16) | 9 (20) | 6 (13) | 1 (9) | 3 (19) | |
| T4 | 17 (14) | 4 (9) | 8 (18) | 2 (18) | 3 (19) | |
| Missing | 6 | 2 | 0 | 4 | 0 | |
| Nodal statusb | 0.01 e | |||||
| Negative | 31 (29) | 7 (17) | 11 (27) | 4 (36) | 9 (64) | |
| Positive | 77 (71) | 35 (83) | 30 (73) | 7 (64) | 5 (36) | |
| Missing | 15 | 5 | 4 | 4 | 2 | |
| NHG (PT) | <0.001 e | |||||
| I | 8 (8) | 7 (18) | 1 (3) | 0 | 0 | |
| II | 50 (51) | 28 (72) | 15 (39) | 6 (60) | 1 (9) | |
| III | 40 (41) | 4 (10) | 22 (58) | 4 (40) | 10 (91) | |
| Missing | 25 | 8 | 7 | 5 | 5 | |
| ER (PT) | <0.001 e | |||||
| Negative | 20 (17) | 1 (2) | 1 (2) | 6 (40) | 12 (75) | |
| Positive | 99 (83) | 43 (98) | 43 (98) | 9 (60) | 4 (25) | |
| Missing | 4 | 3 | 1 | 0 | 0 | |
| PR (PT) | <0.001 e | |||||
| Negative | 37 (32) | 4 (10) | 9 (21) | 10 (67) | 14 (88) | |
| Positive | 80 (68) | 38 (90) | 35 (79) | 5 (33) | 2 (12) | |
| Missing | 6 | 5 | 1 | 0 | 0 | |
| HER2 (PT) | <0.001 e | |||||
| Negative | 89 (86) | 32 (94) | 36 (88) | 7 (50) | 14 (100) | |
| Positive | 14 (14) | 2 (6) | 5 (12) | 7 (50) | 0 | |
| Missing | 20 | 13 | 4 | 1 | 2 | |
| BC subtype (PT) | <0.001 e | |||||
| ER+ HER2− | 75 (73) | 32 (94) | 35 (88) | 4 (29) | 4 (29) | |
| HER2+ (ER+/ER−) | 13 (13) | 2 (6) | 4 (10) | 7 (50) | 0 | |
| ER− HER2− | 14 (14) | 0 | 1 (2) | 3 (21) | 10 (71) | |
| Missing | 21 | 13 | 5 | 1 | 2 | |
| MFI (years) | 0.02 e | |||||
| 0 c | 26 (21) | 7 (15) | 11 (24) | 5 (33) | 3 (19) | |
| >0–3 | 23 (19) | 4 (9) | 8 (18) | 4 (27) | 7 (44) | |
| >3 | 74 (60) | 36 (76) | 26 (58) | 6 (40) | 6 (37) | |
| Number of metastatic sites | 0.70 d | |||||
| 1–2 | 82 (67) | 33 (70) | 30 (67) | 8 (53) | 11 (69) | |
| ≥3 | 41 (33) | 14 (30) | 15 (33) | 7 (47) | 5 (31) | |
| Metastatic site | 0.26 d | |||||
| Non-visceral | 51 (42) | 23 (49) | 19 (42) | 3 (20) | 6 (38) | |
| Visceral | 72 (58) | 24 (51) | 26 (58) | 12 (80) | 10 (62) | |
| Number of CTCs (BL) | 0.32 d | |||||
| <5 | 57 (46) | 25 (53) | 16 (36) | 7 (47) | 9 (56) | |
| ≥5 | 66 (54) | 22 (47) | 29 (64) | 8 (53) | 7 (44) | |
| Missing | 0 | 0 | 0 | 0 | 0 |
| Univariable PFS | Multivariable PFS a | Univariable OS | Multivariable OS a | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | HR (95% CI) | p | n | HR (95% CI) | p | n | HR (95% CI) | p | n | HR (95% CI) | p | |
| PT | 123 | 89 | 123 | 69 | ||||||||
| PAM50 subtype | 0.002 b | 0.007 b | 0.001 b | 0.001 b | ||||||||
| Lum A | 47 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Lum B | 45 | 0.94 (0.61–1.4) | 0.79 | 0.93 (0.54–1.6) | 0.81 | 1.1 (0.66–1.8) | 0.77 | 0.92 (0.48–1.8) | 0.81 | |||
| HER2-E | 15 | 1.1 (0.58–2.0) | 0.82 | 0.88 (0.38–2.0) | 0.77 | 1.0 (0.52–2.1) | 0.92 | 0.77 (0.31–1.9) | 0.57 | |||
| Basal-like | 16 | 2.8 (1.6–5.1) | 0.001 | 3.8 (1.5–9.3) | 0.004 | 3.4 (1.8–6.3) | <0.001 | 4.6 (1.8–11.3) | 0.001 | |||
| LNM | 68 | 55 | 68 | 44 | ||||||||
| PAM50 subtype | 0.05 b | 0.28 b | 0.09 b | 0.17 b | ||||||||
| Lum A | 18 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Lum B | 37 | 1.1 (0.6–1.9) | 0.84 | 0.88 (0.41–1.9) | 0.76 | 0.93 (0.5–1.7) | 0.81 | 1.2 (0.53–2.8) | 0.63 | |||
| HER2-E | 9 | 0.73 (0.3–1.8) | 0.48 | 0.41 (0.13–1.3) | 0.12 | 0.63 (0.23–1.7) | 0.37 | 0.45 (0.13–1.6) | 0.23 | |||
| Basal-like | 4 | 4.2 (1.4–13) | 0.01 | 1.5 (0.37–6.4) | 0.55 | 3.4 (1.1–10.3) | 0.04 | 2.7 (0.64–11.6) | 0.18 | |||
| DM | 74 | 58 | 74 | 42 | ||||||||
| PAM50 subtype | 0.11 b | 0.002 b | 0.91 b | 0.05 b | ||||||||
| Lum A | 7 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Lum B | 41 | 0.60 (0.26–1.4) | 0.22 | 0.26 (0.08–0.80) | 0.02 | 0.77 (0.32–1.9) | 0.56 | 0.46 (0.13–1.6) | 0.22 | |||
| HER2-E | 19 | 1.0 (0.42–2.5) | 0.97 | 0.64 (0.20–2.1) | 0.46 | 0.88 (0.33–2.4) | 0.81 | 1.6 (0.40–6.8) | 0.49 | |||
| Basal-like | 7 | 1.4 (0.46–3.9) | 0.58 | 2.4 (0.54–10.3) | 0.26 | 0.69 (0.21–2.3) | 0.55 | 1.3 (0.24–6.4) | 0.79 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jørgensen, C.L.T.; Larsson, A.-M.; Forsare, C.; Aaltonen, K.; Jansson, S.; Bradshaw, R.; Bendahl, P.-O.; Rydén, L. PAM50 Intrinsic Subtype Profiles in Primary and Metastatic Breast Cancer Show a Significant Shift toward More Aggressive Subtypes with Prognostic Implications. Cancers 2021, 13, 1592. https://doi.org/10.3390/cancers13071592
Jørgensen CLT, Larsson A-M, Forsare C, Aaltonen K, Jansson S, Bradshaw R, Bendahl P-O, Rydén L. PAM50 Intrinsic Subtype Profiles in Primary and Metastatic Breast Cancer Show a Significant Shift toward More Aggressive Subtypes with Prognostic Implications. Cancers. 2021; 13(7):1592. https://doi.org/10.3390/cancers13071592
Chicago/Turabian StyleJørgensen, Charlotte Levin Tykjær, Anna-Maria Larsson, Carina Forsare, Kristina Aaltonen, Sara Jansson, Rachel Bradshaw, Pär-Ola Bendahl, and Lisa Rydén. 2021. "PAM50 Intrinsic Subtype Profiles in Primary and Metastatic Breast Cancer Show a Significant Shift toward More Aggressive Subtypes with Prognostic Implications" Cancers 13, no. 7: 1592. https://doi.org/10.3390/cancers13071592